| This website is regularly reviewed by members of the Scientific and Medical Advisory Board of the MHE Research Foundation. |
Disclaimer: While many find the information useful, it is in no way a substitute for professional
medical care.The information provided here is for educational and informational purposes only. This
website does not engage in the practice of medicine. In all cases we recommend that you consult your
own physician regarding any course of treatment or medicine.
medical care.The information provided here is for educational and informational purposes only. This
website does not engage in the practice of medicine. In all cases we recommend that you consult your
own physician regarding any course of treatment or medicine.
Written consent must be obtained to attach web pages or the files attached to this website.
Please email webmaster.
Please email webmaster.
| Email the webmaster: webmaster@mheresearchfoundation.org Materials on this website are protected by copyright Copyright © 2008 The MHE Research Foundation |
The MHE Research Foundation, we comply with the HONcode standard for health
trust worthy information:By the Health On the Net Foundation. Click here to verify.#
HON Conduct 282463 and is linked on the NIH National Library of Medicine,
Directory of Health Organizations (SIS) website,as well as the link for Patient
Information on The Diseases Database a cross-referenced index of human disease,
and the Intute: health & life sciences a free online service providing access to the
very best Web resources for education and research located in the UK
trust worthy information:By the Health On the Net Foundation. Click here to verify.#
HON Conduct 282463 and is linked on the NIH National Library of Medicine,
Directory of Health Organizations (SIS) website,as well as the link for Patient
Information on The Diseases Database a cross-referenced index of human disease,
and the Intute: health & life sciences a free online service providing access to the
very best Web resources for education and research located in the UK
The MHE Research Foundation is proud to be working with the EuroBoNeT consortium,
a European Commission granted Network of Excellence for studying the pathology
and genetics of bone tumors.
a European Commission granted Network of Excellence for studying the pathology
and genetics of bone tumors.
This file will print 15 pages
| This Guide to chondrosarcoma was authored by DAVIDE DONATI M.D. LUCA SANGIORGI M.D., PH.D., Rizzoli Orthopaedic Institute, Bologna Italy & The MHE Research Foundation. What is chondrosarcoma? |
The term chondrosarcoma is used to define an heterogeneous group of lesions with diverse features and
clinical behavior. Chondrosarcoma is a malignant cancer that results in abnormal bone and cartilage growth.
People who have chondrosarcoma have a tumor growth starting from the medullary canal of a long and flat
bone. However, in some cases the lesion can occur as an abnormal bony type of bump, which can vary in
size and location. Primary chondrosarcoma (or conventional chondrosarcoma) usually develops centrally in a
previously normal bone. Secondary chondrosarcoma is a chondrosarcoma arising from a benign precursor
such as Exostoses, Osteochondromas or Enchondromas. Although rare, chondrosarcoma is the second
most common primary bone cancer.
The malignant cartilage cells begin growing within or on the bone (central chondrosarcoma) or, rarely,
secondarily within the cartilaginous cap of a pre-existing Exostoses (peripheral chondrosarcoma).
clinical behavior. Chondrosarcoma is a malignant cancer that results in abnormal bone and cartilage growth.
People who have chondrosarcoma have a tumor growth starting from the medullary canal of a long and flat
bone. However, in some cases the lesion can occur as an abnormal bony type of bump, which can vary in
size and location. Primary chondrosarcoma (or conventional chondrosarcoma) usually develops centrally in a
previously normal bone. Secondary chondrosarcoma is a chondrosarcoma arising from a benign precursor
such as Exostoses, Osteochondromas or Enchondromas. Although rare, chondrosarcoma is the second
most common primary bone cancer.
The malignant cartilage cells begin growing within or on the bone (central chondrosarcoma) or, rarely,
secondarily within the cartilaginous cap of a pre-existing Exostoses (peripheral chondrosarcoma).
|
It is important to understand the difference between a benign and malignant cartilage tumor.
Chondrosarcoma is a sarcoma, (i.e.) a malignant tumor of connective tissue. A chondroma, is the benign
counterpart. Benign bone tumors do not spread to other tissues and organs, and are not life threatening.
They are generally left alone or cured by surgical removal if they cause symptoms such as tenderness via
pressure on surrounding muscles, tendons or nerves.
Exostoses / Osteochondromas
It is a relatively common lesion and can be solitary or multiple. Multiple osteochondromas occur in multiple
hereditary exostosis, usually arise from the metaphysis near the growth plate of long tubular bones. The
outer layer of the head of the osteochondroma is composed of benign hyaline cartilage varying in thickness
and is delineated peripherally by perichondrium. The cartilage has the appearance of disorganized growth
plate and undergoes enchondral ossification with the newly made bone forming the inner portion of the head
Exostoses usually present as slow growing masses, which can be painful if they impinge on a nerve or if the
stalk is fractured.
What are the different kinds of chondrosarcoma?
The single most important factor to consider when evaluating the malignant potential of a chondrosarcoma is
its “histologic grade”, determined by the appearance of tumor material under the microscope (Donati et al.,
2005; Lee et al., 1999; Marcove et al., 1977; Reith et al., 2003; Springfield et al., 1996; Wang et al., 2001). In
addition to histologic grade chondrosarcomas can be classified by their specific histologic variant (clear cell,
mesenchymal, dedifferentiated). The lower grade variants of chondrosarcoma can often be quite difficult to
differentiate from benign lesions because they have similar appearances on radiographic studies.
Conventional chondrosarcomas are divided into four histologic grades based upon their appearance under a
microscope. The grading is based primarily on nuclear size of tumor cells, nuclear staining (hyperchromasia,
or darker staining of nuclear material) and cellularity (Evans et al., 1977).
Grade I(or “low grade”) tumors most resemble normal cartilage, but may surround areas of lamellar bone
(which is not seen in benign lesions), or show atypical cells including binucleate forms(cells with two nuclei
instead of one).
Grade II (or “intermediate grade”) is more cellular with a greater degree of nuclear atypia,
hyperchromasia and nuclear size (Schiller, 1985).
Grade III (or “high grade”) tumors have significant areas of marked pleomorphism, large cells with more
hyperchromatic nuclei than grade II, occasional giant cells and abundant necrosis. Mitoses are frequently
detected.
The vast majority of chondrosarcoma are Grade I or Grade II. Grade III is rare (Bjornsson et al.,
1998).
Grade IV. Belong to this group the subtype variant called mesenchymal and de-differentiated
chondrosarcomas. De-differentiated chondrosarcomas, along with mesenchymal chondrosarcomas, are
highly malignant, particularly aggressive (i.e., rapidly growing and disturbing surrounding tissues) and carry
with them a poor prognosis.
Chondrosarcoma is a sarcoma, (i.e.) a malignant tumor of connective tissue. A chondroma, is the benign
counterpart. Benign bone tumors do not spread to other tissues and organs, and are not life threatening.
They are generally left alone or cured by surgical removal if they cause symptoms such as tenderness via
pressure on surrounding muscles, tendons or nerves.
Exostoses / Osteochondromas
It is a relatively common lesion and can be solitary or multiple. Multiple osteochondromas occur in multiple
hereditary exostosis, usually arise from the metaphysis near the growth plate of long tubular bones. The
outer layer of the head of the osteochondroma is composed of benign hyaline cartilage varying in thickness
and is delineated peripherally by perichondrium. The cartilage has the appearance of disorganized growth
plate and undergoes enchondral ossification with the newly made bone forming the inner portion of the head
Exostoses usually present as slow growing masses, which can be painful if they impinge on a nerve or if the
stalk is fractured.
What are the different kinds of chondrosarcoma?
The single most important factor to consider when evaluating the malignant potential of a chondrosarcoma is
its “histologic grade”, determined by the appearance of tumor material under the microscope (Donati et al.,
2005; Lee et al., 1999; Marcove et al., 1977; Reith et al., 2003; Springfield et al., 1996; Wang et al., 2001). In
addition to histologic grade chondrosarcomas can be classified by their specific histologic variant (clear cell,
mesenchymal, dedifferentiated). The lower grade variants of chondrosarcoma can often be quite difficult to
differentiate from benign lesions because they have similar appearances on radiographic studies.
Conventional chondrosarcomas are divided into four histologic grades based upon their appearance under a
microscope. The grading is based primarily on nuclear size of tumor cells, nuclear staining (hyperchromasia,
or darker staining of nuclear material) and cellularity (Evans et al., 1977).
Grade I(or “low grade”) tumors most resemble normal cartilage, but may surround areas of lamellar bone
(which is not seen in benign lesions), or show atypical cells including binucleate forms(cells with two nuclei
instead of one).
Grade II (or “intermediate grade”) is more cellular with a greater degree of nuclear atypia,
hyperchromasia and nuclear size (Schiller, 1985).
Grade III (or “high grade”) tumors have significant areas of marked pleomorphism, large cells with more
hyperchromatic nuclei than grade II, occasional giant cells and abundant necrosis. Mitoses are frequently
detected.
The vast majority of chondrosarcoma are Grade I or Grade II. Grade III is rare (Bjornsson et al.,
1998).
Grade IV. Belong to this group the subtype variant called mesenchymal and de-differentiated
chondrosarcomas. De-differentiated chondrosarcomas, along with mesenchymal chondrosarcomas, are
highly malignant, particularly aggressive (i.e., rapidly growing and disturbing surrounding tissues) and carry
with them a poor prognosis.
|
Chondrosarcomas may also be classified by their histologic sub-type. These sub-types include Clear cell,
mesenchymal, and de-differentiated.
a) Clear cell chondrosarcomas are low-grade tumors with significant amounts of glycogen. They typically
involve the proximal portion of femur, tibia or humerus. Histologically, cells have abundant clear cytoplasm
embedded in a loose hyaline cartilaginous matrix and an infiltrative growth pattern. Radiographs show a lytic
defect at epiphyseal end of long bones that is sharply demarcated with sclerotic margins. They carry a low
recurrence rate and a good prognosis with wide resection.
mesenchymal, and de-differentiated.
a) Clear cell chondrosarcomas are low-grade tumors with significant amounts of glycogen. They typically
involve the proximal portion of femur, tibia or humerus. Histologically, cells have abundant clear cytoplasm
embedded in a loose hyaline cartilaginous matrix and an infiltrative growth pattern. Radiographs show a lytic
defect at epiphyseal end of long bones that is sharply demarcated with sclerotic margins. They carry a low
recurrence rate and a good prognosis with wide resection.
|
b) Mesenchymal chondrosarcomas are highly aggressive tumors that are radiographically and
histologically distinct from conventional and dedifferentiated types. They are eccentrically located in bone
and commonly extend into soft tissues. This variant of chondrosarcoma is characterized by a bimorphic
pattern that is composed of highly undifferentiated small round cells (similar to Ewing’s Sarcoma) and islands
of well-differentiated hyaline cartilage. This tumor usually affects young adults and teenagers and shows a
widespread distribution in skeleton. The craniofacial bones, the ribs, the ilium and the vertebrae are the most
common site (Bertoni et al., 1983). The treatment is radical surgery combined with chemotherapy.
c) De-differentiated chondrosarcomas represent about 10% of all chondrosarcomas. The most common
sites of involvement are pelvis bones, femur and humerus. This tumor is a distinct variety of chondrosarcoma
containing two clearly defined components: a well-differentiated cartilage tumor (enchondroma or
chondrosarcoma grade I and II) juxtaposed to a high grade non-cartilaginous sarcoma. The malignant non-
cartilaginous component is most frequently malignant fibrous histiocytoma, osteosarcoma or fibrosarcoma,
although other malignant tumors have been reported as the differentiated component. Radiographically the
tumor produces an ill defined, lytic, intraosseous lesion associated with cortical disruption and extension into
the soft tissues. It is more common in adult aged patients and when possible antiblastic chemotherapy is
advised. Surgical treatment has to be radical.
Who gets chondrosarcoma?
Most chondrosarcomas are low-grade lesions. Low grade means very low attitude to spread out in other
organs and tissues. They are typically seen in adults in their late 20s to 60s. They occur more commonly in
men than women. Chondrosarcoma is not contagious. It cannot be passed on to another person by exposure
to a chondrosarcoma patient. Although specialists are not yet certain what causes chondrosarcoma, there
are several factors that put people at a higher risk. Certain conditions may make people more susceptible to
chondrosarcomas:
a) Enchondromas are benign tumors of hyaline cartilage, they arise within the medullary cavity, or on the
surface of bone, where they are called subperiosteal or juxtacortical chondromas. Enchondromas are the
most common of the intraosseous cartilage tumors, they are usually solitary, located in the metaphyseal
region of tubular bones.
b) Ollier’s Disease (a.k.a multiple enchondromatosis) is a disease of multiple benign bone tumors
(enchondromas) within the bones which cause affected bones to swell. The disease often primarily affects
one side of the body. It is not an inherited disease. Patients have bony swellings, limb shortening and
mechanical difficulties, associated with joint disruption and short stature. The condition usually presents
before age 10. These typically occur in the bone metaphyses and can lead to secondary deformity of the
growth plates. There is a small increased risk of malignant transformation to chondrosarcoma, particularly in
flat bones, during adult life.
c) Maffucci Syndrome is a rare genetic disorder characterized by benign enlargements of cartilage
(enchondromas), bone deformities, and dark, irregularly shaped hemangiomas within the body or on the
skin). The disease manifests early in life, usually around the age of 4 or 5 years, with 25% of cases being
congenital. There is relatively high risk of malignant transformation to chondrosarcoma in adult life
(reportedly 20-30%). Relatively few cases have been published in the English literature.
d) Multiple Hereditary Exostoses (MHE / MO / HME a.k.a., osteochondromatoses) is a hereditary
skeletal disorder in which there are numerous cartilage-capped excrescences (sp) in areas of actively
growing bone (osteochondromas). The condition is genetically heterogeneous, and at least three genes
(ext1 and ext2) have been demonstrated to be involved. The reported risk for malignant transformation to
chondrosarcoma has been from 2% to 5%. The lesions most at risk for malignant transformation are those
occurring near the pelvis, scapula, proximal humerus, proximal femur, and spine. Change in size of the
exostosis or onset of pain in an affected adult is cause for further investigation.
People affected by these conditions are at a higher risk because they usually develop several benign bone
tumors, which have a higher chance of becoming malignant. People with these hereditary conditions who
experience sudden growth spurts or increases in hormone production, such as pregnancy, have a slight
increased risk of a benign bone tumor changing into a chondrosarcoma. These patients should be followed
by a bone tumor specialist for all of their lives. Skeletal x-rays should be taken in adults every 18-24 months.
What is known about the genetics of chondrosarcoma?
As evolving molecular techniques are available, several genotypic and phenotypic markers for
chondrosarcoma have been tested to see if they assist in determining tumor grade prognosis. There is
considerable complexity and heterogeneity in the pathologic and clinical behavior of chondrosarcomas. This
is reflected in the diversity of cytogenetic and molecular genetic characteristics that have been described in
these tumors. Please see Sandberg and Bridge (2003), Sandberg (2004), and Bovee et al. (2005) for a
thorough review.
The genetic changes specific to chondrosarcoma continue to be investigated extensively. Although studies
have not yet established a specific or recurrent karyotypic feature for any of these tumors, different
chondrosarcomas have demonstrated anomalies in several tumor suppressor genes, oncogenes, and
transcription factors, including TP53, RAS, EXT1, EXT2, and Sox9. Available cytogenetic and comparative
genomic hybridization (CGH) studies reveal changes in some chondrosarcomas, but fail to do so in others.
These studies are thus far difficult to interpret.
Based on the available studies, it is likely that chondrosarcomas are generated by a coordinated, multi-step
process involving primarily tumor suppressor genes. In fact, the complexity and variety of genetic changes
seen in chondrosarcomas may indicate several distinct genetic pathways. Some of the same genes may be
involved in each, but the order and manner in which they are affected may differ among chondrosarcomas.
Establishing the genes that initiate the neoplastic processes, and that are subsequently involved along the
pathways leading to chondrosarcoma may lead to therapies addressing these molecular changes, as has
been accomplished for several other sarcomas.
Where in the body are chondrosarcomas usually found?
Chondrosarcomas may develop in any part of the body, but most are commonly found in the pelvis, rib cage,
arms (humerus), shoulder blades (scapula) and legs (proximal femur, tibia). Although any bone can be
affected, the long bones (legs, arms, fingers, toes,) pelvis and shoulder blades are most commonly involved.
Occasionally chondrosarcoma has been found in the spine or skull bones.
It is extremely rare to find chondrosarcoma in any internal organs, but this has been described. If
chondrosarcoma spreads from its primary site (i.e., metastasizes), it usually spreads to the lungs. Metastasis
is rare with low-grade tumors, but has been seen, even up to 10 years after diagnosis (Lee et al., 1999).
About half of grade III and nearly all de-differentiated chondrosarcomas will metastasize.
How does someone with chondrosarcoma feel?
Pain associated with chondrosarcoma is usually in the location of the lesion or adjacent joints, muscles,
tendons, nerves, blood vessels, or other soft tissues. In addition to pain, patients with chondrosarcoma may
notice an enlargement of a bone or limb, changes in their ability to walk normally, or decreased range of
motion in joints near the affected bone. People with benign cartilage tumors (i.e., enchondroma or
osteochondroma) rarely have pain that is caused by the tumor (Marco et al., 2000b). Most patients with a
chondrosarcoma will have pain (Bjornsson et al., 1998; Marco et al., 2000a; Mirra et al., 1985; Murphey et
al., 1996) and many will have swelling. It has been reported that in patients with grade I chondrosarcoma,
60% have night pain or rest pain, 21% have vague regional pain, and only 19% have painless tumors (Marco
et al., 2000a). Rarely, people will discover they have a chondrosarcoma when they develop a fracture
through the tumor (Bjornsson et al., 1998).
Sometimes patients with benign cartilage tumors can have pain caused by something other than the tumor.
For example, a rotator cuff injury can be painful at night and an x-ray might show a cartilage tumor in the
shoulder. It is very important to determine whether pain is being caused by the tumor or by another process.
This difference is vital in the diagnosis and treatment of chondrosarcomas.
What tests are needed to determine if someone has chondrosarcoma?
After a doctor asks questions (a history) and performs a physical examination, he/she may order plain x-rays
to evaluate the area of concern. It can be very difficult for doctors to tell the difference between benign
cartilaginous lesions and low-grade chondrosarcomas on x-rays. Both can demonstrate the classic stippled
calcified appearance of cartilaginous bony lesions (Figure 2). If the hard outside covering of the bone
(cortex) appears to be getting chewed away (endosteal scalloping) there is an increased likelihood that the
tumor has malignant potential, but is not necessarily confirmatory. Features typical of lower grade lesions
include dense calcifications appearing in rings or spicules, uniformly distributed calcifications and eccentric
lobular growth of an intramedullary soft tissue mass. One helpful analysis of chondrosarcoma had endosteal
scalloping of more than 2/3rd of the cortical thickness, whereas only 9% of enchondromas had similar
findings (Murphey et al., 1996).
histologically distinct from conventional and dedifferentiated types. They are eccentrically located in bone
and commonly extend into soft tissues. This variant of chondrosarcoma is characterized by a bimorphic
pattern that is composed of highly undifferentiated small round cells (similar to Ewing’s Sarcoma) and islands
of well-differentiated hyaline cartilage. This tumor usually affects young adults and teenagers and shows a
widespread distribution in skeleton. The craniofacial bones, the ribs, the ilium and the vertebrae are the most
common site (Bertoni et al., 1983). The treatment is radical surgery combined with chemotherapy.
c) De-differentiated chondrosarcomas represent about 10% of all chondrosarcomas. The most common
sites of involvement are pelvis bones, femur and humerus. This tumor is a distinct variety of chondrosarcoma
containing two clearly defined components: a well-differentiated cartilage tumor (enchondroma or
chondrosarcoma grade I and II) juxtaposed to a high grade non-cartilaginous sarcoma. The malignant non-
cartilaginous component is most frequently malignant fibrous histiocytoma, osteosarcoma or fibrosarcoma,
although other malignant tumors have been reported as the differentiated component. Radiographically the
tumor produces an ill defined, lytic, intraosseous lesion associated with cortical disruption and extension into
the soft tissues. It is more common in adult aged patients and when possible antiblastic chemotherapy is
advised. Surgical treatment has to be radical.
Who gets chondrosarcoma?
Most chondrosarcomas are low-grade lesions. Low grade means very low attitude to spread out in other
organs and tissues. They are typically seen in adults in their late 20s to 60s. They occur more commonly in
men than women. Chondrosarcoma is not contagious. It cannot be passed on to another person by exposure
to a chondrosarcoma patient. Although specialists are not yet certain what causes chondrosarcoma, there
are several factors that put people at a higher risk. Certain conditions may make people more susceptible to
chondrosarcomas:
a) Enchondromas are benign tumors of hyaline cartilage, they arise within the medullary cavity, or on the
surface of bone, where they are called subperiosteal or juxtacortical chondromas. Enchondromas are the
most common of the intraosseous cartilage tumors, they are usually solitary, located in the metaphyseal
region of tubular bones.
b) Ollier’s Disease (a.k.a multiple enchondromatosis) is a disease of multiple benign bone tumors
(enchondromas) within the bones which cause affected bones to swell. The disease often primarily affects
one side of the body. It is not an inherited disease. Patients have bony swellings, limb shortening and
mechanical difficulties, associated with joint disruption and short stature. The condition usually presents
before age 10. These typically occur in the bone metaphyses and can lead to secondary deformity of the
growth plates. There is a small increased risk of malignant transformation to chondrosarcoma, particularly in
flat bones, during adult life.
c) Maffucci Syndrome is a rare genetic disorder characterized by benign enlargements of cartilage
(enchondromas), bone deformities, and dark, irregularly shaped hemangiomas within the body or on the
skin). The disease manifests early in life, usually around the age of 4 or 5 years, with 25% of cases being
congenital. There is relatively high risk of malignant transformation to chondrosarcoma in adult life
(reportedly 20-30%). Relatively few cases have been published in the English literature.
d) Multiple Hereditary Exostoses (MHE / MO / HME a.k.a., osteochondromatoses) is a hereditary
skeletal disorder in which there are numerous cartilage-capped excrescences (sp) in areas of actively
growing bone (osteochondromas). The condition is genetically heterogeneous, and at least three genes
(ext1 and ext2) have been demonstrated to be involved. The reported risk for malignant transformation to
chondrosarcoma has been from 2% to 5%. The lesions most at risk for malignant transformation are those
occurring near the pelvis, scapula, proximal humerus, proximal femur, and spine. Change in size of the
exostosis or onset of pain in an affected adult is cause for further investigation.
People affected by these conditions are at a higher risk because they usually develop several benign bone
tumors, which have a higher chance of becoming malignant. People with these hereditary conditions who
experience sudden growth spurts or increases in hormone production, such as pregnancy, have a slight
increased risk of a benign bone tumor changing into a chondrosarcoma. These patients should be followed
by a bone tumor specialist for all of their lives. Skeletal x-rays should be taken in adults every 18-24 months.
What is known about the genetics of chondrosarcoma?
As evolving molecular techniques are available, several genotypic and phenotypic markers for
chondrosarcoma have been tested to see if they assist in determining tumor grade prognosis. There is
considerable complexity and heterogeneity in the pathologic and clinical behavior of chondrosarcomas. This
is reflected in the diversity of cytogenetic and molecular genetic characteristics that have been described in
these tumors. Please see Sandberg and Bridge (2003), Sandberg (2004), and Bovee et al. (2005) for a
thorough review.
The genetic changes specific to chondrosarcoma continue to be investigated extensively. Although studies
have not yet established a specific or recurrent karyotypic feature for any of these tumors, different
chondrosarcomas have demonstrated anomalies in several tumor suppressor genes, oncogenes, and
transcription factors, including TP53, RAS, EXT1, EXT2, and Sox9. Available cytogenetic and comparative
genomic hybridization (CGH) studies reveal changes in some chondrosarcomas, but fail to do so in others.
These studies are thus far difficult to interpret.
Based on the available studies, it is likely that chondrosarcomas are generated by a coordinated, multi-step
process involving primarily tumor suppressor genes. In fact, the complexity and variety of genetic changes
seen in chondrosarcomas may indicate several distinct genetic pathways. Some of the same genes may be
involved in each, but the order and manner in which they are affected may differ among chondrosarcomas.
Establishing the genes that initiate the neoplastic processes, and that are subsequently involved along the
pathways leading to chondrosarcoma may lead to therapies addressing these molecular changes, as has
been accomplished for several other sarcomas.
Where in the body are chondrosarcomas usually found?
Chondrosarcomas may develop in any part of the body, but most are commonly found in the pelvis, rib cage,
arms (humerus), shoulder blades (scapula) and legs (proximal femur, tibia). Although any bone can be
affected, the long bones (legs, arms, fingers, toes,) pelvis and shoulder blades are most commonly involved.
Occasionally chondrosarcoma has been found in the spine or skull bones.
It is extremely rare to find chondrosarcoma in any internal organs, but this has been described. If
chondrosarcoma spreads from its primary site (i.e., metastasizes), it usually spreads to the lungs. Metastasis
is rare with low-grade tumors, but has been seen, even up to 10 years after diagnosis (Lee et al., 1999).
About half of grade III and nearly all de-differentiated chondrosarcomas will metastasize.
How does someone with chondrosarcoma feel?
Pain associated with chondrosarcoma is usually in the location of the lesion or adjacent joints, muscles,
tendons, nerves, blood vessels, or other soft tissues. In addition to pain, patients with chondrosarcoma may
notice an enlargement of a bone or limb, changes in their ability to walk normally, or decreased range of
motion in joints near the affected bone. People with benign cartilage tumors (i.e., enchondroma or
osteochondroma) rarely have pain that is caused by the tumor (Marco et al., 2000b). Most patients with a
chondrosarcoma will have pain (Bjornsson et al., 1998; Marco et al., 2000a; Mirra et al., 1985; Murphey et
al., 1996) and many will have swelling. It has been reported that in patients with grade I chondrosarcoma,
60% have night pain or rest pain, 21% have vague regional pain, and only 19% have painless tumors (Marco
et al., 2000a). Rarely, people will discover they have a chondrosarcoma when they develop a fracture
through the tumor (Bjornsson et al., 1998).
Sometimes patients with benign cartilage tumors can have pain caused by something other than the tumor.
For example, a rotator cuff injury can be painful at night and an x-ray might show a cartilage tumor in the
shoulder. It is very important to determine whether pain is being caused by the tumor or by another process.
This difference is vital in the diagnosis and treatment of chondrosarcomas.
What tests are needed to determine if someone has chondrosarcoma?
After a doctor asks questions (a history) and performs a physical examination, he/she may order plain x-rays
to evaluate the area of concern. It can be very difficult for doctors to tell the difference between benign
cartilaginous lesions and low-grade chondrosarcomas on x-rays. Both can demonstrate the classic stippled
calcified appearance of cartilaginous bony lesions (Figure 2). If the hard outside covering of the bone
(cortex) appears to be getting chewed away (endosteal scalloping) there is an increased likelihood that the
tumor has malignant potential, but is not necessarily confirmatory. Features typical of lower grade lesions
include dense calcifications appearing in rings or spicules, uniformly distributed calcifications and eccentric
lobular growth of an intramedullary soft tissue mass. One helpful analysis of chondrosarcoma had endosteal
scalloping of more than 2/3rd of the cortical thickness, whereas only 9% of enchondromas had similar
findings (Murphey et al., 1996).

Figure 2: Plain radiographs of a low-grade cartilage lesion in a distal femur bone.
|

More aggressive (malignant) tumors may show more telling signs of malignancy on x-ray. This includes
adaptive changes such as expansion and/or thickening of the cortex and expansion of the surrounding soft
tissues (Murphey et al., 1996; Unni, 1996). Findings suggestive of higher grade include faint amorphous
calcifications, large areas lacking calcifications and a concentrically growing soft tissue mass.
Perhaps the most reliable radiographic finding when differentiating between benign and malignant lesions is
the recognition of change in radiographic appearance over time. In particular, there may be more endosteal
scalloping and destruction of the cortex or a decrease in the calcifications with more malignant tumors. If
there is no change in the appearance of a benign cartilage tumor on radiographs over time, it is appropriate
for the doctor to continue to recommend watchful waiting and repeat x-rays at a later visit.
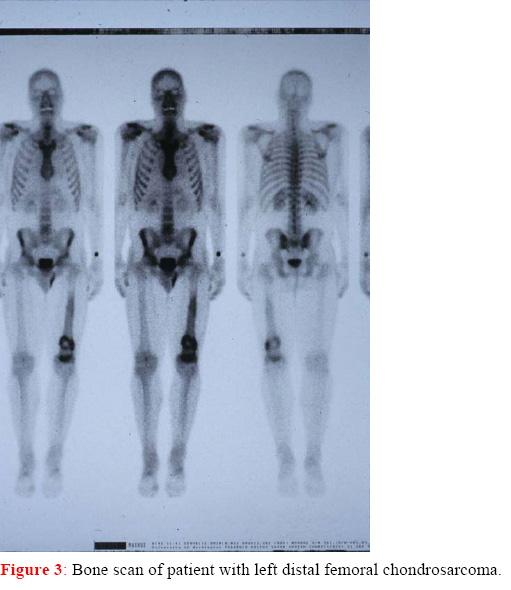
A bone scan of the entire body can also be helpful in differentiating between benign and malignant tumors,
and in identifying whether more than one bone is involved (although multiple bone involvement is rare with
chondrosarcomas). This test works by injecting a small amount of radioactive material into the blood stream
and taking images using a gamma camera to detect uptake of radioactive material. Lesions demonstrated on
bone scan can be compared to internal controls (Murphey et al., 1996). Those lesions demonstrating a
higher degree of uptake are more likely to be of higher histologic grade. However, most Enchondromas and
Exostoses / Osteochondroma exhibit some radioisotope uptake, and some will erroneously
appear as malignancy. Great caution should therefore be used in drawing conclusions from bone scan
results, but these results can add to the overall picture, and better inform the decision making process.
adaptive changes such as expansion and/or thickening of the cortex and expansion of the surrounding soft
tissues (Murphey et al., 1996; Unni, 1996). Findings suggestive of higher grade include faint amorphous
calcifications, large areas lacking calcifications and a concentrically growing soft tissue mass.
Perhaps the most reliable radiographic finding when differentiating between benign and malignant lesions is
the recognition of change in radiographic appearance over time. In particular, there may be more endosteal
scalloping and destruction of the cortex or a decrease in the calcifications with more malignant tumors. If
there is no change in the appearance of a benign cartilage tumor on radiographs over time, it is appropriate
for the doctor to continue to recommend watchful waiting and repeat x-rays at a later visit.
A bone scan of the entire body can also be helpful in differentiating between benign and malignant tumors,
and in identifying whether more than one bone is involved (although multiple bone involvement is rare with
chondrosarcomas). This test works by injecting a small amount of radioactive material into the blood stream
and taking images using a gamma camera to detect uptake of radioactive material. Lesions demonstrated on
bone scan can be compared to internal controls (Murphey et al., 1996). Those lesions demonstrating a
higher degree of uptake are more likely to be of higher histologic grade. However, most Enchondromas and
Exostoses / Osteochondroma exhibit some radioisotope uptake, and some will erroneously
appear as malignancy. Great caution should therefore be used in drawing conclusions from bone scan
results, but these results can add to the overall picture, and better inform the decision making process.

Recently, there has been some research into the use of a specialized radiographic test called fluorine-18
fluorodeoxyglucose positron emission tomography (FDG PET) for grading of tumors in patients with
chondrosarcoma (Aoki et al., 1999; Brenner et al., 2004). This test is not yet available at all centers, but may
become a useful tool for tumor grading and prediction of outcome in chondrosarcoma patients. This may
hence allow for identification of patients at high risk for local relapse or metastatic disease.
Axial computed tomography (CT) can assist in determining the extent of bony destruction, and in better
delineating bony architecture. CT will also help in better understanding intralesional calcifications. As with
plain radiographs, disappearance or change in the nature of calcifications with repeat scanning can be
suggestive of malignancy.
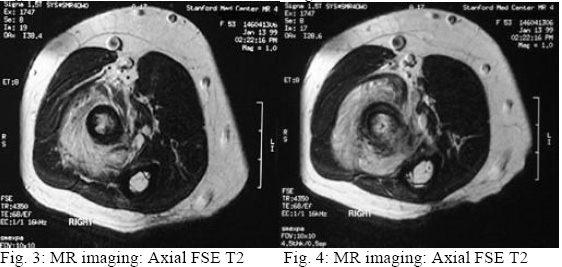
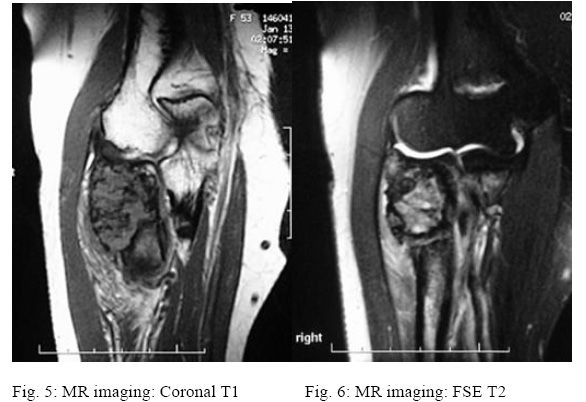
Magnetic Resonance Imaging (MRI) can be helpful in differentiating between benign and malignant lesions
in several ways. First, the degree to which the tumor fills the medullary canal can be helpful (Figure 4).
Greater than 90% medullary involvement can be suggestive of chondrosarcoma, while the absence of 90%
medullary involvement of non-contiguous areas of cartilage within the bone can suggest the presence of an
enchondroma (Colyer et al., 1993). In addition, the timing and progression of gadolinium contrast
enhancement patterns may help direct a clinician toward or away from a diagnosis of malignancy (Geirnaerdt
et al., 2000). Early enhancement (within 10 seconds of arterial enhancement) may be seen in
chondrosarcoma but not in enchondroma. Many surgeons consider MRI critical for surgical planning because
it can illustrate the extent of tumor involvement in bone and soft tissues.
What if a chondrosarcoma is suspected?
If chondrosarcoma is suspected, two additional (staging) tests will usually be done to determine whether the
tumor has spread. These include: 1) a computerized tomography (CT) scan of the lungs; and, 2) a total
body bone scan. The results of these staging studies help physicians determine treatments and outcomes
(prognosis). Blood tests are generally not helpful in making the diagnosis, although they can be used to
make sure that there is not another process going on, such as infection or a different malignant process.
After all of these tests are performed, a sample of the tumor (biopsy) is sometimes necessary to figure out if
the problem is truly chondrosarcoma. Most biopsies for chondrosarcoma are achieved by surgical excision
(i.e., complete removal of the tumor) of the lesion rather than through incisional biopsy (i.e., surgery to
remove only part of the tumor for diagnostic evaluation).
What will a biopsy tell the patient and the doctor?
When fresh tissue from a chondrosarcomas is viewed under a microscope after a biopsy, it is generally not
difficult to identify a clear distinction between normal host tissue and the malignant tissue. However, with
higher-grade tumors, more aggressive margins may have more malignant tissue, and have infiltrating
satellite components. They will exhibit heterogeneous gross properties including lobulated areas of chalky
calcific admixture, regions of firm translucent unmineralized gray cartilage and relatively low vascularity.
Higher-grade tumors tend to have areas of necrosis and degenerative material as well (Enneking, 1983).
fluorodeoxyglucose positron emission tomography (FDG PET) for grading of tumors in patients with
chondrosarcoma (Aoki et al., 1999; Brenner et al., 2004). This test is not yet available at all centers, but may
become a useful tool for tumor grading and prediction of outcome in chondrosarcoma patients. This may
hence allow for identification of patients at high risk for local relapse or metastatic disease.
Axial computed tomography (CT) can assist in determining the extent of bony destruction, and in better
delineating bony architecture. CT will also help in better understanding intralesional calcifications. As with
plain radiographs, disappearance or change in the nature of calcifications with repeat scanning can be
suggestive of malignancy.
Magnetic Resonance Imaging (MRI) can be helpful in differentiating between benign and malignant lesions
in several ways. First, the degree to which the tumor fills the medullary canal can be helpful (Figure 4).
Greater than 90% medullary involvement can be suggestive of chondrosarcoma, while the absence of 90%
medullary involvement of non-contiguous areas of cartilage within the bone can suggest the presence of an
enchondroma (Colyer et al., 1993). In addition, the timing and progression of gadolinium contrast
enhancement patterns may help direct a clinician toward or away from a diagnosis of malignancy (Geirnaerdt
et al., 2000). Early enhancement (within 10 seconds of arterial enhancement) may be seen in
chondrosarcoma but not in enchondroma. Many surgeons consider MRI critical for surgical planning because
it can illustrate the extent of tumor involvement in bone and soft tissues.
What if a chondrosarcoma is suspected?
If chondrosarcoma is suspected, two additional (staging) tests will usually be done to determine whether the
tumor has spread. These include: 1) a computerized tomography (CT) scan of the lungs; and, 2) a total
body bone scan. The results of these staging studies help physicians determine treatments and outcomes
(prognosis). Blood tests are generally not helpful in making the diagnosis, although they can be used to
make sure that there is not another process going on, such as infection or a different malignant process.
After all of these tests are performed, a sample of the tumor (biopsy) is sometimes necessary to figure out if
the problem is truly chondrosarcoma. Most biopsies for chondrosarcoma are achieved by surgical excision
(i.e., complete removal of the tumor) of the lesion rather than through incisional biopsy (i.e., surgery to
remove only part of the tumor for diagnostic evaluation).
What will a biopsy tell the patient and the doctor?
When fresh tissue from a chondrosarcomas is viewed under a microscope after a biopsy, it is generally not
difficult to identify a clear distinction between normal host tissue and the malignant tissue. However, with
higher-grade tumors, more aggressive margins may have more malignant tissue, and have infiltrating
satellite components. They will exhibit heterogeneous gross properties including lobulated areas of chalky
calcific admixture, regions of firm translucent unmineralized gray cartilage and relatively low vascularity.
Higher-grade tumors tend to have areas of necrosis and degenerative material as well (Enneking, 1983).
|

As both benign and malignant cartilage lesions can share certain clinical and histological characteristics,
pathologists will often consider the patient’s history when interpreting specimens. Permeation of cortical
and/or medullary bone is an important characteristic of conventional chondrosarcoma that the pathologist
can use to separate it from Enchondroma / Osteochondroma. The decision by the orthopaedic oncologist
for definitive treatment is based upon the areas of highest concern for malignancy. Lesions appearing more
aggressive clinically and radiographically must be widely resected without biopsy to avoid contamination of
healthy tissue, which would likely necessitate an additional surgery. However, this remains controversial. The
surgeon decision is based on history and progression of the lesion referred by the patients and confirmed by
the previous examinations. The histological grade is sometimes necessary to plan a preoperative
chemotheraphy in IV grade chondrosarcomas. Or on the other hand to plan a more conservative surgery in
border line lesions (benign, low-grade)
What are the current treatments for chondrosarcoma?
For benign-appearing, asymptomatic cartilage tumors (i.e., enchondroma), patients are usually followed with
clinical evaluation and sequential x-rays 3, 6 and then 12 months apart. This is continued unless there is a
change in clinical examination findings or the radiographic appearance of the lesion at different points in
time. Symptomatic enchondromas as well as exostoses /osteochondroma (i.e., those that cause pain,
discomfort, or are disfiguring but do not show indications of malignancy) can be treated with a relatively non-
invasive procedure. Enchondromas can be curetted out from inside the medullary canal of the bone with
placement of a bone graft, while exostoses can be excised from the bone surface. Fractures through the
tumor (called a pathologic fracture) can be treated with either concurrent or staged treatment of both the
fracture and the lesion if there is concern over the risk of recurrent pathologic fracture.
Surgical resection remains the primary and most successful means of treating chondrosarcomas. The
decision regarding the extent of surgical resection and adjuvant therapy is dependent upon the clinical and
histologic characteristics of the lesion. Optimal treatment for low-grade chondrosarcoma remains a dilemma
for surgical oncologists, but no chemotherapy or radiation is indicated. For higher-grade tumors, with a worse
prognosis for recurrence and metastasis, adjuvant therapies may be considered.
pathologists will often consider the patient’s history when interpreting specimens. Permeation of cortical
and/or medullary bone is an important characteristic of conventional chondrosarcoma that the pathologist
can use to separate it from Enchondroma / Osteochondroma. The decision by the orthopaedic oncologist
for definitive treatment is based upon the areas of highest concern for malignancy. Lesions appearing more
aggressive clinically and radiographically must be widely resected without biopsy to avoid contamination of
healthy tissue, which would likely necessitate an additional surgery. However, this remains controversial. The
surgeon decision is based on history and progression of the lesion referred by the patients and confirmed by
the previous examinations. The histological grade is sometimes necessary to plan a preoperative
chemotheraphy in IV grade chondrosarcomas. Or on the other hand to plan a more conservative surgery in
border line lesions (benign, low-grade)
What are the current treatments for chondrosarcoma?
For benign-appearing, asymptomatic cartilage tumors (i.e., enchondroma), patients are usually followed with
clinical evaluation and sequential x-rays 3, 6 and then 12 months apart. This is continued unless there is a
change in clinical examination findings or the radiographic appearance of the lesion at different points in
time. Symptomatic enchondromas as well as exostoses /osteochondroma (i.e., those that cause pain,
discomfort, or are disfiguring but do not show indications of malignancy) can be treated with a relatively non-
invasive procedure. Enchondromas can be curetted out from inside the medullary canal of the bone with
placement of a bone graft, while exostoses can be excised from the bone surface. Fractures through the
tumor (called a pathologic fracture) can be treated with either concurrent or staged treatment of both the
fracture and the lesion if there is concern over the risk of recurrent pathologic fracture.
Surgical resection remains the primary and most successful means of treating chondrosarcomas. The
decision regarding the extent of surgical resection and adjuvant therapy is dependent upon the clinical and
histologic characteristics of the lesion. Optimal treatment for low-grade chondrosarcoma remains a dilemma
for surgical oncologists, but no chemotherapy or radiation is indicated. For higher-grade tumors, with a worse
prognosis for recurrence and metastasis, adjuvant therapies may be considered.

|
In the past, wide resection was considered the method of choice for all chondrosarcomas. Unfortunately,
these tumors are frequently found in regions such as the pelvis or proximal long bones, where aggressive
surgical management may endanger adjacent vital organs and structures or compromise limb function. Thus,
less aggressive approaches such as marginal excision and extended intralesional excision with margin
expansion using adjuncts such as phenol or cryotherapy have received increasing attention with a national
study underway to investigate efficacy. Most surgical oncologists prefer limb salvage techniques with bone
graft and prosthetics, preserving the function of the limb. Amputation is still used in advanced disease or as a
last option.
these tumors are frequently found in regions such as the pelvis or proximal long bones, where aggressive
surgical management may endanger adjacent vital organs and structures or compromise limb function. Thus,
less aggressive approaches such as marginal excision and extended intralesional excision with margin
expansion using adjuncts such as phenol or cryotherapy have received increasing attention with a national
study underway to investigate efficacy. Most surgical oncologists prefer limb salvage techniques with bone
graft and prosthetics, preserving the function of the limb. Amputation is still used in advanced disease or as a
last option.
|
While rigorous evidence-based criteria are presently lacking, individual centers may have their own criteria
and algorithms for surgical decision-making. In general, benign lesions should be treated conservatively,
while high-grade malignancies should be treated aggressively with complete resection. If surgical margins are
not clear on histologic evaluation of the tissue after resection of an intermediate- or high-grade lesion, wider
surgical resection and possibly bone and/or joint prosthesis may be necessary.
Clinical Trials
Optimal treatment for low-grade chondrosarcoma remains a dilemma for surgical oncologists. For patients
who have developed pulmonary metastatic disease, treatment in a clinical trial at a Sarcoma center, or with
conventional chemotherapy, if appropriate for the patient, may be indicated. At the time of this writing, there
is a multi-center, international trial evaluating the diagnosis and treatment of low grade chondrosarcoma and
a trial dealing with advanced chondrosarcomas sponsored by the
National Institutes of Health, the Southwest Oncology Group, and The American College of Surgeons
Oncology Group, Sarcoma Alliance for Research Through Collaboration (SARC), Patient Advocacy
Groups
Intralesional Resection in Treating Patients With Chondrosarcoma of the Bone
This Phase II trial is currently recruiting patients. Intralesional resection is a less invasive type of surgery for
chondrosarcoma of the bone and may have fewer side effects and improve recovery. The purpose of this
trial is to study how well intralesional resection works in treating patients with low-grade chondrosarcoma of
the bone. Patients undergo intralesional resection (curettage with high-speed burr). Patients then receive
local adjuvant treatment comprising of liquid nitrogen, phenol, alcohol, or argon beam to the excision site.
The bone cavity is then filled with either polymethyacrylate cement or a bone graft (allograft or homograft).
Patients may also have a metal plate installed at the wound site.
Patients are followed every 3 months for 1 year and then every 6 months for 4 years. A total of 60 patients
will be accrued for this study within 30-60 months. Patients 18 years of age and older are eligible. This trial is
taking place at centers in Arkansas, Colorado, Florida, Michigan, Minnesota, Missouri, New Mexico, Oregon,
Utah, and Washington.
Pemetrexed Disodium in Treating Patients With Recurrent and Unresectable or Metastatic
Chondrosarcoma
This Phase II trial is currently recruiting patients. Pemetrexed disodium (Alimta) is a potent new antifolate
which inhibits many folate-dependent reactions that are essential for cell proliferation. Its primary target is
thymidylate synthase but it also inhibits folate-dependent enzymes involved in purine synthesis. Cells that are
resistant to antifolates are generally less resistant to pemetrexed, irrespective of the mechanism of
resistance. Pemetrexed has shown good activity in preclinical models with human tumor cells and xenografts.
In the majority of clinical trials of pemetrexed, the dose-limiting toxic effect is neutropenia; other side-effects
are mostly gastrointestinal. Preclinical studies indicate that the toxic effects of pemetrexed can be reduced by
dietary folate, resulting in an improved therapeutic index. Low folate status is also associated with higher
levels of toxicity in patients.
As a single agent pemetrexed has shown good activity against non-small-cell lung cancer, squamous-cell
carcinoma of head and neck, colon cancer, and breast cancer, and it appears to be particularly active in
combination with cisplatin against non-small-cell lung cancer and mesothelioma. The purpose of this trial is to
study how well pemetrexed disodium works in treating patients with recurrent and unresectable or metastatic
chondrosarcoma. Patients are stratified according to prior chemotherapy (yes vs. no). The treatment outline
is as follows. Patients receive pemetrexed disodium IV over 10 minutes on day 1. Courses repeat every 21
days* in the absence of disease progression or unacceptable toxicity (NOTE: *The duration of course 1 is 28
days; the duration of all subsequent courses is 21 days). Beginning 7 days before the first dose of
pemetrexed disodium and continuing until 21 days after the completion of pemetrexed disodium, patients
receive cyanocobalamin (vitamin B-12) intramuscularly once every 63 days and oral folic acid once daily.
Patients achieving a complete response (CR) receive 2 additional courses beyond CR. Patients achieving a
confirmed partial response (PR) that is resectable, proceed to surgical resection and then receive 2
additional courses of therapy after recovering from surgery. Patients achieving a confirmed PR that is not
resectable continue treatment in the absence of disease progression or unacceptable toxicity. After
completion of study treatment, patients are followed every 3 months until disease progression and then every
6 months for up to 5 years. A total of 40-75 patients (20-40 in the previously treated stratum and 20-35 in
the previously untreated stratum) will be accrued for this study within 20-37.5 months. Patients 18 years of
age and older are eligible. This trial is taking place at centers in California, Illinois, Kansas, Missouri,
Montana, North Carolina, South Carolina, and Wyoming.
The effects of ciprofloxacin and paclitaxel on metastatic and recurrent chondrosarcoma
Edward J. Fox, MD, Jesse T. Torbert, MD, Anne-Marie Martin, PhD, Arthur P. Staddon, MD, Joseph L.
Finstein, MD, and Richard D. Lackman, MD
Department of Orthopaedic Surgery, The University of Pennsylvania, Philadelphia, PA
Currently, the only treatment available for recurrent/metastatic chondrosarcoma is further surgical resection.
Fluoroquinolones have shown toxicity in immature cartilage, inducing apoptosis and inhibiting the
proliferation of human chondrosarcoma cells. Since previous studies suggested that ciprofloxacin and
paclitaxel act synergistically in slowing the growth of chondrosarcoma in vitro, we investigated their effects on
human recurrent/metastatic chondrosarcoma.
Four patients received oral ciprofloxacin (750 mg twice daily) and intravenous paclitaxel (90 mg/m²) for 6–8
weeks of each cycle. Patient 1 remained stable 32.8 weeks after initiation of treatment. Patient 2 showed a
60% decrease in tumor growth but progressed by 10.3 weeks. Patient 3 progressed over 9 weeks, remained
stable for 16 months, and then progressed after treatment with paclitaxel was discontinued. Patient 4 had
three lesions: the recurrent lesion progressed despite treatment, showing an 8% increase in growth; one
metastatic lesion remained stable (18 weeks), and the second metastatic lesion progressed. Gene
expression profiling of normal articular cartilage and human chondrosarcoma cells exposed to ciprofloxacin
showed differential expression of the genes DDX5, MYST2, ISGF3, APC, RPL3, EIF4G2, and ERH, all of
which are involved in cell proliferation, cell-cycle regulation, or apoptosis.
Where is the best place to go to receive appropriate treatment?
Patients with chondrosarcoma are best treated at major Sarcoma centers with specialized diagnostic and
treatment facilities and the availability of Musculoskeletal Tumor Specialists or Orthopedic Oncologists.
Because this, like many other bone cancers, are not common, it is often a good idea to seek an opinion from
a major cancer center that has a wide experience in treating bone cancers. A major sarcoma center will offer
an organized group of doctors and other health care professionals who work together to provide the best
treatment options and recovery. If your primary care physician suspects chondrosarcoma, a simple referral to
an orthopedic doctor may not be adequate. Be sure that you are referred to an orthopaedic oncologist or
"bone cancer specialist."
What are the chances for cure and survival from chondrosarcoma?
In general, the prognosis for chondrosarcoma depends on the grade of the tumor and the attainment of
complete excision of the tumor and other conditions the patient has such as diabetes, lupus, and clotting and
coagulation problems. For lower grade chondrosarcomas, prognosis is very good after adequate excision.
There is a low incidence of pulmonary metastasis if the primary lesion is widely resected. Metastasis to other
bones can occur, but is much less common. Dedifferentiated chondrosarcoma have a uniformly poor
prognosis.
and algorithms for surgical decision-making. In general, benign lesions should be treated conservatively,
while high-grade malignancies should be treated aggressively with complete resection. If surgical margins are
not clear on histologic evaluation of the tissue after resection of an intermediate- or high-grade lesion, wider
surgical resection and possibly bone and/or joint prosthesis may be necessary.
Clinical Trials
Optimal treatment for low-grade chondrosarcoma remains a dilemma for surgical oncologists. For patients
who have developed pulmonary metastatic disease, treatment in a clinical trial at a Sarcoma center, or with
conventional chemotherapy, if appropriate for the patient, may be indicated. At the time of this writing, there
is a multi-center, international trial evaluating the diagnosis and treatment of low grade chondrosarcoma and
a trial dealing with advanced chondrosarcomas sponsored by the
National Institutes of Health, the Southwest Oncology Group, and The American College of Surgeons
Oncology Group, Sarcoma Alliance for Research Through Collaboration (SARC), Patient Advocacy
Groups
Intralesional Resection in Treating Patients With Chondrosarcoma of the Bone
This Phase II trial is currently recruiting patients. Intralesional resection is a less invasive type of surgery for
chondrosarcoma of the bone and may have fewer side effects and improve recovery. The purpose of this
trial is to study how well intralesional resection works in treating patients with low-grade chondrosarcoma of
the bone. Patients undergo intralesional resection (curettage with high-speed burr). Patients then receive
local adjuvant treatment comprising of liquid nitrogen, phenol, alcohol, or argon beam to the excision site.
The bone cavity is then filled with either polymethyacrylate cement or a bone graft (allograft or homograft).
Patients may also have a metal plate installed at the wound site.
Patients are followed every 3 months for 1 year and then every 6 months for 4 years. A total of 60 patients
will be accrued for this study within 30-60 months. Patients 18 years of age and older are eligible. This trial is
taking place at centers in Arkansas, Colorado, Florida, Michigan, Minnesota, Missouri, New Mexico, Oregon,
Utah, and Washington.
Pemetrexed Disodium in Treating Patients With Recurrent and Unresectable or Metastatic
Chondrosarcoma
This Phase II trial is currently recruiting patients. Pemetrexed disodium (Alimta) is a potent new antifolate
which inhibits many folate-dependent reactions that are essential for cell proliferation. Its primary target is
thymidylate synthase but it also inhibits folate-dependent enzymes involved in purine synthesis. Cells that are
resistant to antifolates are generally less resistant to pemetrexed, irrespective of the mechanism of
resistance. Pemetrexed has shown good activity in preclinical models with human tumor cells and xenografts.
In the majority of clinical trials of pemetrexed, the dose-limiting toxic effect is neutropenia; other side-effects
are mostly gastrointestinal. Preclinical studies indicate that the toxic effects of pemetrexed can be reduced by
dietary folate, resulting in an improved therapeutic index. Low folate status is also associated with higher
levels of toxicity in patients.
As a single agent pemetrexed has shown good activity against non-small-cell lung cancer, squamous-cell
carcinoma of head and neck, colon cancer, and breast cancer, and it appears to be particularly active in
combination with cisplatin against non-small-cell lung cancer and mesothelioma. The purpose of this trial is to
study how well pemetrexed disodium works in treating patients with recurrent and unresectable or metastatic
chondrosarcoma. Patients are stratified according to prior chemotherapy (yes vs. no). The treatment outline
is as follows. Patients receive pemetrexed disodium IV over 10 minutes on day 1. Courses repeat every 21
days* in the absence of disease progression or unacceptable toxicity (NOTE: *The duration of course 1 is 28
days; the duration of all subsequent courses is 21 days). Beginning 7 days before the first dose of
pemetrexed disodium and continuing until 21 days after the completion of pemetrexed disodium, patients
receive cyanocobalamin (vitamin B-12) intramuscularly once every 63 days and oral folic acid once daily.
Patients achieving a complete response (CR) receive 2 additional courses beyond CR. Patients achieving a
confirmed partial response (PR) that is resectable, proceed to surgical resection and then receive 2
additional courses of therapy after recovering from surgery. Patients achieving a confirmed PR that is not
resectable continue treatment in the absence of disease progression or unacceptable toxicity. After
completion of study treatment, patients are followed every 3 months until disease progression and then every
6 months for up to 5 years. A total of 40-75 patients (20-40 in the previously treated stratum and 20-35 in
the previously untreated stratum) will be accrued for this study within 20-37.5 months. Patients 18 years of
age and older are eligible. This trial is taking place at centers in California, Illinois, Kansas, Missouri,
Montana, North Carolina, South Carolina, and Wyoming.
The effects of ciprofloxacin and paclitaxel on metastatic and recurrent chondrosarcoma
Edward J. Fox, MD, Jesse T. Torbert, MD, Anne-Marie Martin, PhD, Arthur P. Staddon, MD, Joseph L.
Finstein, MD, and Richard D. Lackman, MD
Department of Orthopaedic Surgery, The University of Pennsylvania, Philadelphia, PA
Currently, the only treatment available for recurrent/metastatic chondrosarcoma is further surgical resection.
Fluoroquinolones have shown toxicity in immature cartilage, inducing apoptosis and inhibiting the
proliferation of human chondrosarcoma cells. Since previous studies suggested that ciprofloxacin and
paclitaxel act synergistically in slowing the growth of chondrosarcoma in vitro, we investigated their effects on
human recurrent/metastatic chondrosarcoma.
Four patients received oral ciprofloxacin (750 mg twice daily) and intravenous paclitaxel (90 mg/m²) for 6–8
weeks of each cycle. Patient 1 remained stable 32.8 weeks after initiation of treatment. Patient 2 showed a
60% decrease in tumor growth but progressed by 10.3 weeks. Patient 3 progressed over 9 weeks, remained
stable for 16 months, and then progressed after treatment with paclitaxel was discontinued. Patient 4 had
three lesions: the recurrent lesion progressed despite treatment, showing an 8% increase in growth; one
metastatic lesion remained stable (18 weeks), and the second metastatic lesion progressed. Gene
expression profiling of normal articular cartilage and human chondrosarcoma cells exposed to ciprofloxacin
showed differential expression of the genes DDX5, MYST2, ISGF3, APC, RPL3, EIF4G2, and ERH, all of
which are involved in cell proliferation, cell-cycle regulation, or apoptosis.
Where is the best place to go to receive appropriate treatment?
Patients with chondrosarcoma are best treated at major Sarcoma centers with specialized diagnostic and
treatment facilities and the availability of Musculoskeletal Tumor Specialists or Orthopedic Oncologists.
Because this, like many other bone cancers, are not common, it is often a good idea to seek an opinion from
a major cancer center that has a wide experience in treating bone cancers. A major sarcoma center will offer
an organized group of doctors and other health care professionals who work together to provide the best
treatment options and recovery. If your primary care physician suspects chondrosarcoma, a simple referral to
an orthopedic doctor may not be adequate. Be sure that you are referred to an orthopaedic oncologist or
"bone cancer specialist."
What are the chances for cure and survival from chondrosarcoma?
In general, the prognosis for chondrosarcoma depends on the grade of the tumor and the attainment of
complete excision of the tumor and other conditions the patient has such as diabetes, lupus, and clotting and
coagulation problems. For lower grade chondrosarcomas, prognosis is very good after adequate excision.
There is a low incidence of pulmonary metastasis if the primary lesion is widely resected. Metastasis to other
bones can occur, but is much less common. Dedifferentiated chondrosarcoma have a uniformly poor
prognosis.

Summary
Cartilaginous lesions of the human skeleton exist on a continuum spanning from the completely benign
embryonic inclusion, to the dangerously aggressive neoplastic process. In order to determine the appropriate
treatment for each individual lesion, musculoskeletal oncologists must take into account the clinical,
radiographic and histologic characteristics of the tumor.
It is important for patients to seek treatment for these tumors at a Sarcoma center with availability of
specialists possessing a sound understanding of these lesions and a firm grasp of the evolving treatment
options. The health care team at these centers will keep patients informed about the details of the treatment
course in both the short and long term. Understanding and recognizing the spectrum of appearances of the
various types of chondrosarcoma allow improved patient assessment and are vital for optimal clinical
management including diagnosis, biopsy, staging, treatment and prognosis. As more advanced molecular
tools for predicting tumor behavior are developed, more sophisticated means of diagnosing and treating
these tumors will be developed and put into use.
Where else can one learn about Chondrosarcoma?
Steve Dunn's Cancer Guide provides a very useful starting point for undertaking investigations into cancer
and cancer-related issues on the Internet. Among other things discussed is how to research the medical
literature and how to use and access medical databases and online resources, explains the medical research
cycle, where to get medical references and describes the various types of papers in the medical literature,
and how to find and use a medical library.
Interested readers are encouraged to continue their investigations into chondrosarcoma by examining the
resources at the websites listed below:
Chondrosarcoma by Dr. Geoff Hide on the eMedicine.com website
The Doctor's Doctor chondrosarcoma webpage
Liddy Shriver Sarcoma Initiative
Connective Tissue Oncology Society
EuroBoNet
Cartilaginous lesions of the human skeleton exist on a continuum spanning from the completely benign
embryonic inclusion, to the dangerously aggressive neoplastic process. In order to determine the appropriate
treatment for each individual lesion, musculoskeletal oncologists must take into account the clinical,
radiographic and histologic characteristics of the tumor.
It is important for patients to seek treatment for these tumors at a Sarcoma center with availability of
specialists possessing a sound understanding of these lesions and a firm grasp of the evolving treatment
options. The health care team at these centers will keep patients informed about the details of the treatment
course in both the short and long term. Understanding and recognizing the spectrum of appearances of the
various types of chondrosarcoma allow improved patient assessment and are vital for optimal clinical
management including diagnosis, biopsy, staging, treatment and prognosis. As more advanced molecular
tools for predicting tumor behavior are developed, more sophisticated means of diagnosing and treating
these tumors will be developed and put into use.
Where else can one learn about Chondrosarcoma?
Steve Dunn's Cancer Guide provides a very useful starting point for undertaking investigations into cancer
and cancer-related issues on the Internet. Among other things discussed is how to research the medical
literature and how to use and access medical databases and online resources, explains the medical research
cycle, where to get medical references and describes the various types of papers in the medical literature,
and how to find and use a medical library.
Interested readers are encouraged to continue their investigations into chondrosarcoma by examining the
resources at the websites listed below:
Chondrosarcoma by Dr. Geoff Hide on the eMedicine.com website
The Doctor's Doctor chondrosarcoma webpage
Liddy Shriver Sarcoma Initiative
Connective Tissue Oncology Society
EuroBoNet